Gastric Sleeve Surgery
(Sleeve Gastrectomy)
The most commonly performed bariatric surgery in the United States — a powerful, permanent solution with a strong safety profile and outstanding long-term results.
What Happens During a Gastric Sleeve
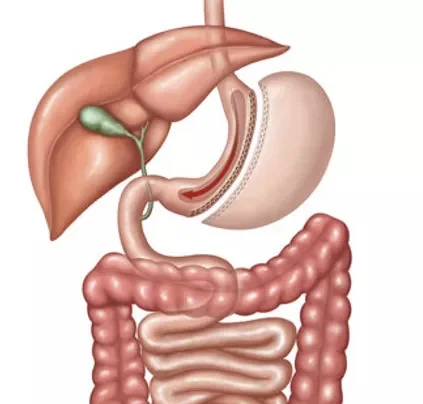
The gastric sleeve removes approximately 70–80% of the stomach — specifically the larger, "stretchy" section that expands when you eat large meals. What remains is a narrow, banana-shaped tube (the "sleeve") that holds dramatically less food.
Originally developed as the first step in a two-stage duodenal switch procedure for very high-BMI patients, surgeons noticed so many patients lost enough weight with the sleeve alone that they never needed the second step. It's now the most performed bariatric procedure in the United States.
Unlike bypass procedures, the sleeve does not reroute the intestines — making it technically simpler with a lower risk profile. It still produces meaningful metabolic and hormonal effects, particularly by reducing ghrelin (the hunger hormone) production.
Strong hunger and portion control
Significantly reduces the volume of food you can eat. Ghrelin reduction means you feel less hungry overall — a key advantage over non-surgical methods.
Simpler surgery, lower short-term risk
No intestinal connections (anastomoses) means a technically simpler procedure with a strong safety profile — shorter hospital stay, faster recovery.
Convertible to bypass, SADI-S, or DS
If you need more weight loss down the road, the sleeve can be converted to a gastric bypass, SADI-S, or duodenal switch — keeping your surgical options open.
Moderate metabolic effect
More than a gastric band, less than a bypass — the sleeve produces meaningful improvement in diabetes, blood pressure, and cholesterol for most patients.
Important Considerations After Sleeve Surgery
The gastric sleeve gives you restriction and hunger control — but it does not eliminate food cravings the way bypass does. Here's what every patient should understand going in.
Food selection is still your responsibility
Unlike gastric bypass, the sleeve doesn't cause "dumping syndrome" with sugar, so patients are less likely to feel sick from eating poorly. This means food choices matter more — you must actively improve your diet to achieve the best results.
Not reversible — permanent stomach reduction
Once the stomach section is removed, it cannot be put back. This is a permanent, irreversible change. However, the sleeve can be revised or converted to other procedures if needed in the future.
Long-term data (10+ years) still emerging
As a standalone procedure, the sleeve is newer than bypass — so very long-term outcome data is still being gathered. Current data is excellent, but patients should be aware this is an evolving picture.
Possible GERD / heartburn development
Some patients develop or worsen acid reflux (GERD) years after sleeve surgery. If reflux is already a significant issue for you, discuss this with your surgeon — gastric bypass may be a better option.
Weight regain risk over time
There is some evidence that sleeve patients may experience higher rates of weight regain after 5–10 years compared to bypass. Consistent follow-up care and lifestyle habits are essential to long-term success.
Daily vitamin supplements are simpler
Because the intestines aren't rerouted, absorption is mostly preserved. Supplement requirements are simpler than bypass — typically just a multivitamin, vitamin D, and calcium.
Who Is the Ideal Gastric Sleeve Candidate?
BMI 35–50 — the sleeve is most effective in this range
Patients who prefer no intestinal rerouting — simpler anatomy, easier reversal to alternative procedures
No significant acid reflux / GERD — patients without GERD do best; bypass is preferred if reflux is severe
Committed to dietary improvement — since the sleeve doesn't restrict food selection the way bypass does, lifestyle changes are crucial
Want to preserve future surgical options — can be converted to bypass, SADI-S, or DS if more weight loss is needed
Severe acid reflux / GERD — gastric bypass resolves reflux in 90%+ of patients and is strongly preferred
BMI 50+ — SADI-S or duodenal switch typically delivers superior results at very high BMIs
Severe Type 2 diabetes — bypass and SADI-S have higher diabetes remission rates (~75–90% vs ~60%)
Every case is unique. Book a consultation — our surgeons will give you an honest recommendation.
Gastric Sleeve vs. Other Procedures
| Factor | Gastric Sleeve | Gastric Bypass | SADI-S | Duodenal Switch |
|---|---|---|---|---|
| Excess Weight Loss | 60–70% | 65–75% | 80–85% | 80–90% |
| Diabetes Remission | ~60% | ~75% | ~90% | ~95% |
| Acid Reflux | May worsen | Resolves 90%+ | Mostly improves | Mostly improves |
| Intestinal Bypass | No | Yes | Yes (~50%) | Yes (~75%) |
| Hospital Stay | 1–2 days | 2–3 days | 2–3 days | 2–4 days |
| Convertible Later | Yes ✓ | Technically yes | No | No |
Ready to Find Out If the Gastric Sleeve Is Right for You?
Our board-certified bariatric surgeons will evaluate your BMI, health history, and goals — and give you an honest recommendation with no pressure.
Serving Corpus Christi, South Texas, Victoria, Laredo, McAllen & surrounding areas